
Vive la vaccination!
Have you ever had a vaccination injection at the doctor’s office or at school? Then you’ve probably heard about the basics – how the injection helps ‘train’ your immune system by presenting it with a weakened version of an illness so that it’s ready to fight the real thing.
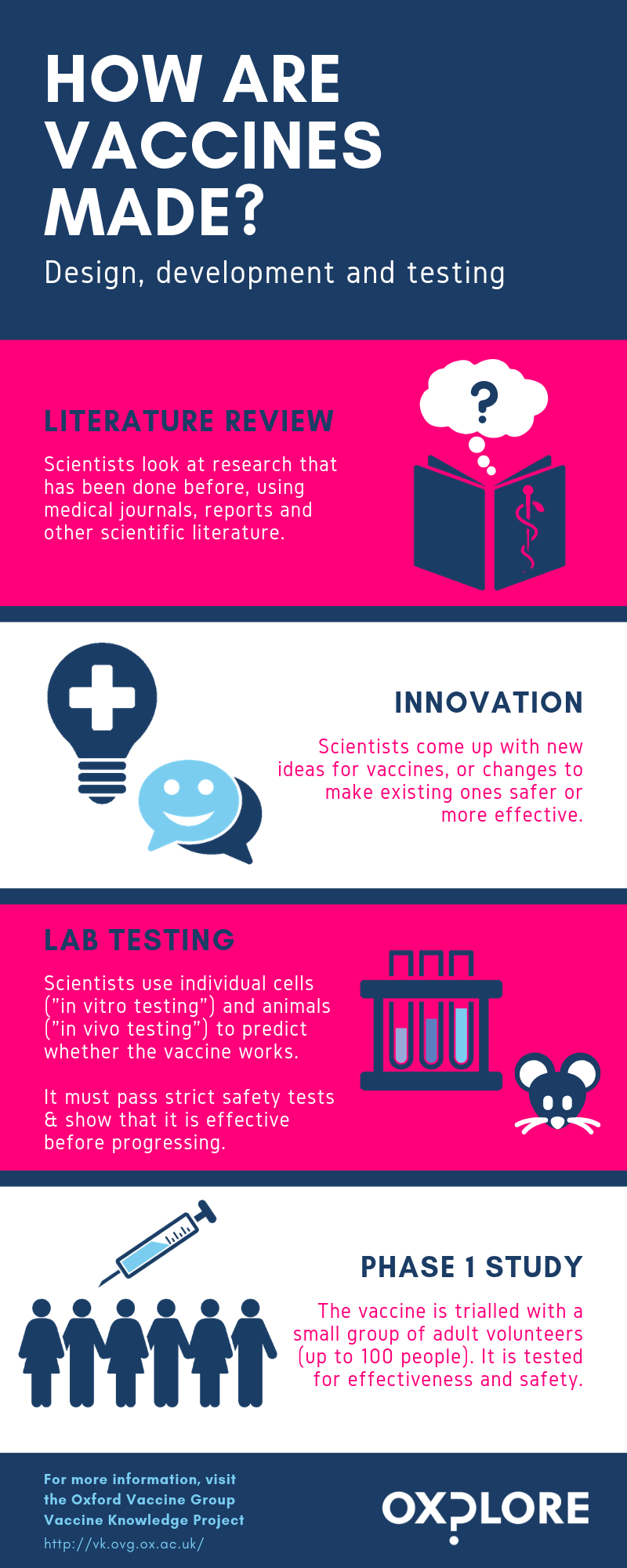
How are vaccines made and tested?
Understandably, people are often concerned to know how well vaccines have been tested before they are used on human beings. In the UK, the standard for testing and monitoring of vaccines is higher than it is for most other medicines, because they are one of the few medical treatments given to healthy people (mainly healthy children). This means that the level of acceptable risk is much lower than it might be for a cancer treatment, for example.
This graphic shows all the stages that a new vaccine needs to pass through before it can be given to people. It can take many years for a vaccine to pass through all the stages – for example, in the case of the MenB vaccine for meningitis (a dangerous bacterial infection which attacks the brain, blood and spinal cord), it took nearly 20 years from the first idea to the vaccine being licensed for use.
What impact has the invention of vaccination had on diseases?
Case study: Smallpox
Smallpox was a viral disease caused by the variola virus. It caused an illness which had lots of different symptoms – including making people develop a rash of pustules (large, painful fluid-filled sores) covering their entire body. On average, it took the rash 24 hours to cover the body and an additional three weeks for pustules to grow in size, form crusts and eventually fall off. The rate of death for the more common and dangerous variola major strain of the virus was estimated to be around 30%. People who survived would often be marked for life with scarring from the pustules, which could be very severe.
Smallpox had been around since at least the time of the Ancient Egyptians, and there was no successful treatment other than letting the disease run its course. However, some groups of people in China and India practiced variolation – a technique of introducing people, especially young children, to the smallpox virus in the form of liquid from the pustules of ill people or dried pustule scabs which were inhaled in controlled quantities. This usually caused the person to develop a milder form of the disease, which then gave them immunity (although sometimes they unfortunately caught the full-blown version and died). At the end of the 18th century, the British doctor Edward Jenner extended this technique to pioneer the first ever true vaccination, using the related cowpox virus to protect patients. His discovery was based in part on information about variolation that Lady Mary Montague, the wife of a British ambassador, had sent back from Istanbul in the 1710s (Read more).
Tip: Jenner invented the smallpox vaccination in 1796 -- using a calculator, find the average share of smallpox deaths in the ten years before this (1786-1796) and the ten years after (1797-1807). Then compare these to the ten years after that (1808-1818). What happens over time?
Footnote: Note the big jump in smallpox deaths in 1871 – this is an anomaly linked to the Franco-Prussian War of 1870, when transporting French prisoners of war who hadn't been vaccinated contributed to a smallpox epidemic which killed more than 500,000 people across Europe (Source).
Be aware that this data comes from a time when other standards, like cleanliness and access to trained health care workers, were also on the rise, so these factors might be playing a role too!
Following World War II, the World Health Organisation declared a resolution to eradicate smallpox around the world and launched its Intensified Smallpox Eradication Programme in 1967. The last known case ‘in the wild’ was reported in Somalia in 1977. Since then, scientists estimate that this has saved around 5 million people’s lives per year.
So why would people not want to be vaccinated?
Given all this, why would some people not want themselves or their children to be vaccinated? One relatively recent reason is a piece of discredited research published in the 1990s by former physician Andrew Wakefield, linking the MMR (Measles, Mumps and Rubella) vaccine with autism. Although this research was found to be based on false data and retracted by the medical journal which published it (and Wakefield has since been barred from practising medicine) the idea had taken hold in many people’s minds. At around this time many people also became concerned about the ethics of the big pharmaceutical companies manufacturing the vaccines, and about whether they were allowing their business interests to override their duty to protect people’s wellbeing.
A 95% immunisation rate is required to maintain herd protection, but after Wakefield’s ‘research’ was published immunisation rates dipped below 80% in the UK, and measles infections rose (source).
The UK immunisation rate for MMR is now back up over 90%, but it has been dropping over the past five years (2015-2019), and the UK recently lost its World Health Organisation status as a "measles-free" country (source).
A short history of mental health
In the past, people thought about mental illness in a variety of different ways. These might vary according to people’s cultures and the places in which they were living – for example, at some points in European history people might have associated the symptoms of some psychiatric illnesses with witchcraft or the idea of being possessed by demons, and unfortunately sometimes those affected were persecuted or even killed.
At the court of Sultan An-Nasir Salah ad-Din Yusuf ibn Ayyub in Cairo during the 1100s some people thought ‘madness’ had something to do with possession by spirits, but they also believed that it could be caused by an imbalance of ‘humours’ or elements in the body. Some doctors also seem to have had a rudimentary understanding of the idea of depression, which they called ‘melancholy’. Muslim, Jewish and Christian doctors working at the Sultan’s court believed that people who were suffering from ‘melancholy’ needed pleasant company, music and the opportunity to engage with things they found interesting. They created herbal treatments and suggested activities such as reading good books on philosophy and religion to help. Learn more in this lecture by Daniel Nicolae.
The image above was painted into a book around 1185, and may be a portrait of Sultan An-Nasir Salah ad-Din Yusuf ibn Ayyub. Credit: Public domain.
.jpg){kind=link}
In London during the 1600s and 1700s, people with serious mental illnesses were often locked up against their will in Bethlem Royal Hospital.
This had been built as a very luxurious and modern hospital for people who were too ill to take care of themselves - but it quickly went downhill as the building became run-down and the hospital began to raise extra money by allowing visitors to tour the hospital in order to look at the patients, and even laugh at them and taunt them. The name “Bethlem” became shortened to “Bedlam”, and due to the poor conditions in which the patients lived “Bedlam” eventually became a synonym for any place or situation that was disordered, noisy and chaotic. Read more.
The image below shows a patient, James Norris (sometimes known as William Norris), being held in restraints at “Bedlam” during the early 1800s. Images like this led people to campaign for better conditions for the patients. Credit: William Norris, shackled on his bed at Bedlam: Wellcome Collection.
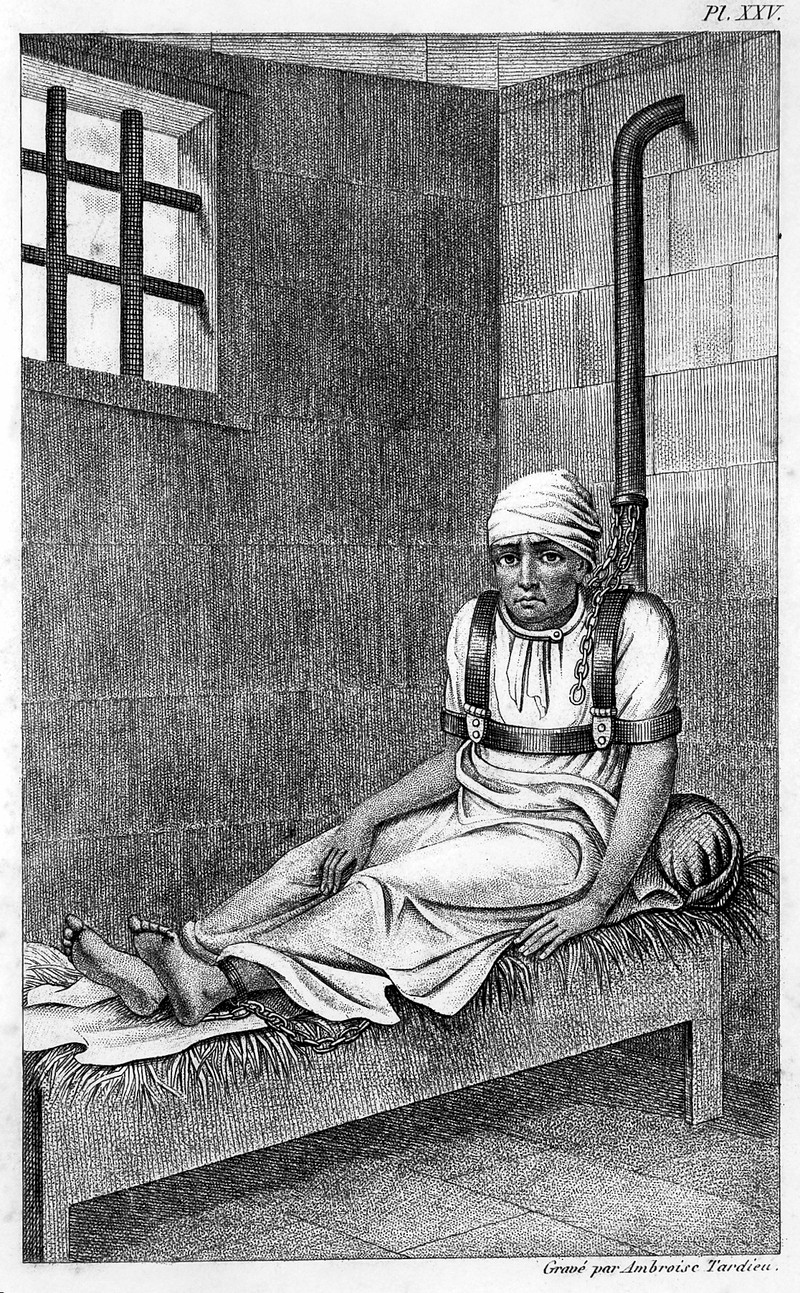
What do you think? Did “Bedlam” make life better for people with serious mental illnesses, or did it make their lives worse? Consider that the alternatives to being confined to hospital may have been living on the street with no access to food or shelter.
During the Victorian period, people started to think a bit differently about mental health. Two new inventions - the railway and the ‘penny post’ which allowed people to send each other letters quickly and often - made many people feel that the pace of life was ‘speeding up’. They suddenly had to cope with lots of new information arriving in the post (some people got up to 12 mail deliveries a day!) and the ability to travel to different towns and cities very quickly. Many people worried about the impact of these stresses on their “nerves”, by which they meant their ability to cope with everyday situations and anxiety.
This might sound a bit familiar - people nowadays often report feeling similarly bombarded by emails and social media notifications or exhausted by aeroplane travel. The Diseases of Modern Life Project at Oxford University has spent the last few years studying images, documents and statistics from the past to learn more about how Victorian people understood the impact of stress on mental health.
How are things changing?
Nowadays, there is an increasing shift in the media to share people's mental health experiences and to create greater awareness of what support is available - helping to make those who are suffering from mental illness feel less isolated.
For example, the UK-based charity Comic Relief led a campaign in 2018 which involved a mix of celebrities and members of the general public sharing their experiences. The campaign suggested that mental illness can affect anyone at any stage of their life, and so we all need to take care of our mental health. The message that unites the speakers' experiences is the importance of talking to someone and not suffering in silence.
https://www.youtube.com/watch?v=tv82K_M7o5A
At the same time, more and more schools are considering how mindfulness training and activities can be included in the support they provide to students. Researchers at the University of Oxford have been leading studies into this very area via the MYRIAD project. The project is based on the knowledge that childhood and the teenage years are a vulnerable time for the start of mental illness: 75% of mental disorders begin before the age of 24, and half by age 15 (Kessler et al., 2005). The Department of Health (2011) recommends that “By promoting good mental health and intervening early… we can help to prevent mental illness from developing and mitigate [reduce] its effects when it does”. With this in mind, the MYRIAD team have taken an 8-week Mindfulness course which is known to be effective in preventing depression and promoting mental health in adults, and adapted it to work and appeal to teenagers in a (mainstream) classroom setting. For a definition of mindfulness, check out our article in our ‘Are we getting unhappier?’ big question.
The role of digital technology and mental health
Through her work on the Be-GOOD project, Prof. Ilina Singh (Department of Psychiatry) studies young people’s ethical and moral understandings of key issues related to mental health.
These include what it means to: experience personal agency (i.e. a sense of control over your choices); be a good citizen; lead a good life, and behave well. As part of this, the research team have focused on building digital tools to investigate young people’s moral and ethical attitudes to mental health innovations such as mental health apps. Another area of interest is young people's opinions on predictive technologies that could uncover the risk of mental ill health before symptoms have appeared.
Digital approaches to mental health service delivery could be seen as supporting young people in understanding their own mental health. On the other hand, these could be seen as over-generalising mental health challenges, or even encouraging young people to think they have a mental illness. This raises ethical tensions. For example, how should we balance the good that can come from better and more acceptable routes of access to mental health services for young people against the harms to personal identity and privacy that can accompany sharing deeply personal data on-line?

It also raises questions about what role a mental health app should play: should it replace or assist a doctor? Who is responsible for the ‘care’ offered and outcomes… Is it the app designers? The person who recommended the app in the first place? The app user? The technology itself? And how should new users be encouraged to join? Those suffering from mental health conditions may be especially vulnerable, and so apps and their designers should be mindful of the power they might have in shaping users’ thinking and behaviours. This is particularly important since the world of online mental health support is still a relatively unregulated space. And so Prof. Ilina Singh stresses the importance of taking what we know about what does and doesn’t work well with the face-to-face therapist-patient relationship, and trying to translate this to create online mental health tools (source).
What does the future hold?
Over time we are learning more and more about mental health, including how to treat mental illnesses and how to help patients manage their symptoms. In particular, researchers are interested in finding ways to support young people early on in settings such as school to prevent them from developing mental health problems in the future. Some researchers view digital apps as a potential method to effectively reach out to (some) young people. Alongside this, the media is giving a greater voice to those who face mental health problems through charity campaigns and beyond. This helps to break down the stigma (negative feelings) of mental illness while improving awareness.
That’s not to say that more work isn’t needed… In fact, the (UK) Youth Index, which measures young people's levels of happiness and confidence across various aspects of their lives, is at an all-time low compared to when this information was first collated 10 years ago (source). But in terms of developing our overall understanding and awareness of mental health, active steps are being taken.